HIV TESTING AND SURVEILLANCE Presentation Presidential AIDS Advisory Panel Meeting By Eleni Papadopoulos & Val Turner
3 & 4 July 2000
This is the presentation made to the Presidential Panel in Johannesberg on Monday July 3rd 2000 by the Perth Group. It addressed the topic HIV Testing and Surveillance. The presentation has been edited to include extra data pointing to a cellular origin for the HIV proteins.We believe AIDS exists and there is a correlation between AIDS and the antibody tests. And that sex plays a role in the development of a positive antibody test and AIDS. We do not claim to have proof that HIV does not exist but we do have misgivings with the proof that HIV has been isolated. Finally, despite the fact that we have been slaving away at the AIDS problem for almost 20 years, we admit we may be wrong.
The Durban Declaration asserts that patients with acquired immune deficiency syndrome, regardless of where they live, are infected with HIV. The basis of this statement is that AIDS patients possess antibodies which react with an assortment of proteins deemed unique to HIV. To perform antibody tests the first thing one must do is obtain the HIV proteins. Since viruses and the cells in which one is obliged to grow viruses share the same biochemical constituents, to define and recover the virus proteins the virus particles must be purified.
Mass Production and Purification
"...analysis of the proteins demands mass production and purification" -- Luc Montagnier 1997.Purification of retroviruses is achieved by banding culture material in sucrose density gradients. A drop of culture supernatant is placed on top of a column of sucrose solution of increasing density in a test tube. The tube is spun at high speeds for several hours and during this time the retroviral particles, if present, travel though the gradient until they encounter sucrose of the same density. When they do, they stop and thus concentrate.
In 1983 Professor Montagnier claimed to have discovered HIV based on this method. Material which banded at 1.16 gm/ml he and his colleagues called pure virus. One of the three proteins in this material, which reacted with AIDS patient serum, was said to be a unique, HIV p24 protein. Although it was long considered mandatory to take an electron micrograph to prove that gradient purified material contained retroviral particles and nothing else but retrovirus particles, no such EM was ever published. This caveat, which is really no more than commonsense, to exclude that there may not actually be a retrovirus, had in fact been listed as requirement by two of Montagniers co-authors a decade earlier. Despite this omission, such banded material has been used by all HIV researchers to obtain proteins, and RNA, to use a diagnostic agents to prove HIV infection.
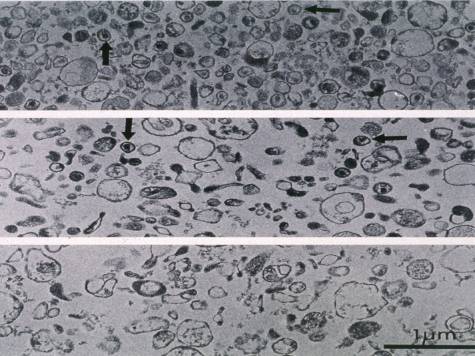
The first EMs of what was called purified HIV did not appear until fourteen years afterwards. This EM and the one following were published in March 1997 in Virology. This EM is from a Franco/German collaboration which includes Hans Gelderblom from the Koch Institute in Berlin. The second is from the US National Cancer Institute. In both slides the upper two EMs are density gradient purified HIV and the lower EM a density gradient of a non-infected culture. Obviously, whatever these appearances represent, nothing has been purified. The authors admit this. They also claim that in the infected cultures, amongst all the contaminating cellular material, there are a small number of particles which are a retrovirus and are HIV. But they dont provide any proof. In fact in this slide there are two HIV particles in the non-infected material but none of the particles in this or the NCI slide
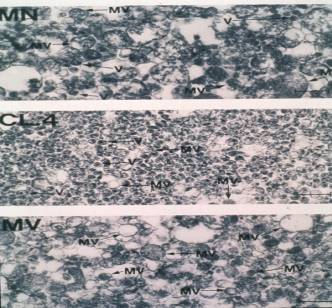
have the appearance of retroviruses, let alone a specific retrovirus. For example, the HIV particles in this slide are two and half times the diameter of any known retrovirus. This is equivalent to a 15 foot man. To account for the appearances on these EMs the authors adopted the term co-purification. (You like your whisky neat but when the barman forgets he leans over and tells you not to worry because the ginger ale co-purifies).
"I repeat, we did not purify" Luc Montagnier, Pasteur Institute Interview July 1997Of significant interest, in a 1997 interview, Professor Montagnier said he did not purify his 1983 HIV. And that despite a Roman effort, he was unable to find any particles with the morphology typical of retroviruses in his gradient purified virus. This interview was published by Huw Christie in Continuum and a video tape copy is sitting on the table in front of where I am sitting. (This video was later given to the South African Government after obtaining permission from its copyright owner).
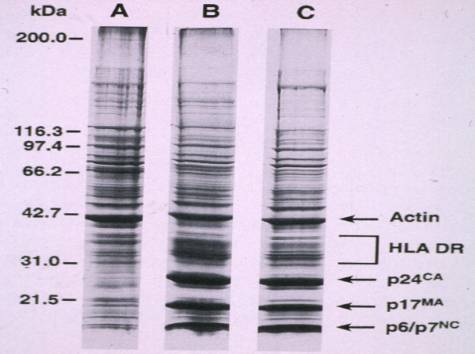
If you perform a protein electrophoresis on the infected and non-infected gradient purified material, you get this picture. The only differences between lane A , which is non-infected, and lanes B and C, which are, are quantitative, not qualitative. The bands labeled HIV down the bottom of lanes B and C can also be seen, although not strongly, in the non-infected specimen. This could be explained by the different culture conditions. The infected cultures originate from AIDS patients who are highly oxidised and these cultures are chemically stimulated. And this material used to infect these cultures already contains these proteins whereas the lane A cultures are cultured on their own. This same data was published in an earlier paper by the same authors but without labels indicating viral proteins. We asked the senior author how they proved the strong bands were HIV proteins. His reply did not mention any such proof but merely informed us that the labels were added at the suggestion of the editor to better orientate the reader. Independent data show that the proteins labelled p24 and p18 have been found in a wide variety of uninfected human tissues using AIDS sera and monoclonal antibodies to the so called HIV proteins. And where are the rest of the so called HIV proteins in this purified virus? Where are p41 and p65 and p120 and p160? In other words, these data are better explained by HIV proteins being not viral but cellular. In fact there are much other, independent data proving that all the HIV proteins are cellular or, at the very least, non-specific.
In 1983 Montagnier declared that his p45 (now p41) protein is cellular actin which contaminated his purified virus. He reiterated this in 1996. Others have proven that actin is a component of pure HIV. HIV researchers accept that the p160 protein is present only in cell cultures, not HIV itself. But p160 is one of the HIV antigens used in the Western blot and is presumably also present in the HIV ELISA. This means the method used to obtain the HIV proteins for the WB does not use pure virus as we can now readily accept given the EMs of purified HIV. But there is another explanation.
In 1989 Pinter and his colleagues did a chemical analysis of the so called HIV glycoproteins present in the WB and found that p120 and p160 are oligomers of p41. They went so far as to warn that Confusion over the identification of these bands has resulted in incorrect conclusions some clinical specimens may been identified erroneously as seropositive
The non-specificity of the p24 antigen test is so obvious that it is accepted by no less an authority on HIV testing than Philip Mortimer and his colleagues from the UK Public Health Laboratory Service, "Experience has shown that neither HIV culture nor tests for p24 antigen are of much value in diagnostic testing. They may be insensitive and/or non-specific". p24 arises in cultures of non-infected individuals and in fact the highest levels of the p24 HIV antigen are reported not from AIDS patients but from no risk, non-HIV-infected organ transplant recipients.
The HIV Proteins
Henderson (1987) studied the p30-32 and p34-36 of "HIV purified by double banding" in sucrose density gradients. Comparison with the amino-acid sequences of these proteins with Class II histocompatability DR proteins proved that "the DR alpha and beta chains appeared to be identical to the p34-36 and p30-32 proteins respectively Cellular origin also acknowledged by other HIV experts such as Arthur (1995).
AIDS sera as well as monoclonal antibodies to the HIV p18 protein bind to a wide variety of tissues from non-AIDS, non-risk, non antibody positive patients and, if we look at the normal human placenta in a little more detail,
Faulk and Labarrere (1991) studied immunocytochemical reactivity using poly- and monoclonal antibodies. Placentae from 25 normal term pregnancies were collected by vaginal delivery...Antigens gp120 and p17 were identified in normal chorionic villi Antigen p24 in villous mesenchymal cells...localized to HLA-DR positive cells
Thus, using antibody probes including monoclonals, three of the HIV specific proteins show up in the placentas of non-HIV-infected women.
Thus, if gradient purified infected material consists of the same proteins as uninfected material, and does not contain retroviral particles, and is not pure, then it is difficult to see how anyone can refer to this material as purified HIV. And use it for diagnostic purposed to pronounce humans infected with a particular lethal retrovirus, HIV.
Well, regardless of the origin of these proteins, AIDS patients most certainly have antibodies that react with these proteins and these reactions correlate with either having AIDS or developing and dying of AIDS. Or being in a risk group. Of this there can be no doubt. The problem for the Perth group, is how to explain this. Well we can only suggest an explanation. Thanks to Kashala and Muller and others we know that antibodies to mycobacteria and fungi such as Candida albicans bind to the proteins present in the HIV antibody test kits. And mycobacteria and fungal diseases comprise about 90% of AIDS diagnoses. Thus some, perhaps quite a lot, of the reactivity might be explained on this basis. AIDS patients have a plethora of autoantibodies and this may explain further reactivity. And under the guise of the immune activation that accompanies AIDS, we can not discount non-specific antibody production and other cross-reactivities. But the problem for us all, is whether these reactions are caused by infection with an AIDS causing retrovirus. And is this all the time, some of the time or never? Is there anything we do to resolve this conundrum? Yes there is. We can walk humbly up to Mother Nature and ask for her help. She will tell you the only way to answer this question is to use a gold standard.
Use the HIV gold standard. Compare the antibody reactions with the virus. Until you do that youre just staring at entrails.
Unfortunately, HIV isolation is problematic in the extreme. When you analyse the detail, at best HIV isolation consists of a series of non-specific phenomena. Measurement of reverse transcription, detection of particles in culture fluids, antibody/antigen reactions all have non-retroviral, non-infectious causes. But we can appreciate that twenty years ago, under such intense pressure to find a cause for AIDS, scientists may have been compelled to interpret these phenomena as proof of isolation of a retrovirus. Nowadays, what is called HIV isolation, is detection of a p24 protein in cultures with an antibody. This is not isolation of a virus and even if it were, scientists cannot use a subset of some antibody/antigen reactions as a gold standard for the complete set.
So, what I have presented thus far are some of the data which have led our group in Perth to question whether presently available data justify the Durban declaration that that HIV exists in all AIDS patients.
Currently available HIV antibody tests are extraordinarily accurate, both in terms of sensitivity (the ability of the test to give a positive finding when a subject is truly HIV-infected) and specificity (the ability of the test to give a negative finding when a subject is truly HIV-free). -- NIAID Web site
What does the majority have to offer to support their view? At the suggestion of the Moderators, we took a look at the NIAID website. And here is quotation from that site asserting that the HIV antibody tests are extraordinarily accurate for diagnosing HIV infection.
Please allow me at this point to make a small diversion. To tell you about the Royal Perth Hospital Department of Emergency Medicine apple pie test. We use this to try and explain the basics of test parameters to our residents. In a vain effort to try and get them to order less tests. This came about because one of my colleagues who has what can only be described as an outstanding passion for apple pies. He works late, lives a little out of town and always gets home after dark. A few years ago noticed that whenever his wife cooked an apple pie, the light over the chookhouse [hen coop in South Africa] was switched on. So he began keeping diary and after a couple of years came up with these data.
Pie in Oven No Pie Light On 80 10 Light Off 2 640 82 650
Days 732 Pies 82 One every 9 days Sensitivity 97.6% Specifity 98.5% If there was a pie the light was almost always on. If there was no pie it was hardly ever on. So you can see this is a very good test. Its sensitivity and specificity are equal to what Gallo claimed for his 1985 HIV ELISA.. These data also illustrate another point. You dont need to know or even begin to understand the relationship between the indicator system, in this case the chookhouse light, and what the test is telling you. All that matters is how these two variables, in their on or off states, map on to this grid.
Disease No disease Positive Negative If the test is highly sensitive and specific, all the numbers should be in the grey rectangles and there should be zeros or very low numbers in the white rectangles.
So, if the WHO are right that the HIV antibody tests are highly sensitive and specific, it should be a simple matter to discover the appropriate data in one of the 120,000 AIDS papers published thus far.
HIV No HIV Positive Negative It should include two columns marked HIV and no-HIV, two rows marked positive and negative and the right set of numbers.
Assay Name (Manufacturer) Global Panel Sensitivity Specificity Detect HIV I + II 100% 97.4% Cambridge 99.6% 99.7% Abbott 3rd generation HIV 100% 100% One of the two references to the WHO statement lists the sensitivities and specificities of 34 different brands of ELISA tests. Ive only put in three. But there are no independent data on how the infection status of the individuals whose serums make up the global panel was determined.
"The panel included 332 HIV negative specimens and 203 sera positive for HIV-1 and 60 positive for HIV-2 specimens"The WHO is using one antibody test as a gold standard for another. Not suprisingly, there is a high degree of concordance but it doesnt get us beyond antibodies reacting with proteins of highly questionable origin. This is not what we want to know. This is what we already know.
AIDS Blood Donors HIV Pos. 86 19 HIV Neg. 2 795 88 814
Sensitivity 97.73% Specificity 97.67% In 1985 Gallo published the results of an ELISA test he evaluated as a serological assay for exposure to HIV. To do this he assumed all AIDS patients infected with HIV and no blood donors infected with HIV. Many others have done the same thing. There are three problems here. Firstly, patients have AIDS because they have a positive antibody test. So you are in effect comparing the current antibody tests with a previous antibody test. In other words, exactly what the WHO did. Second, this method precludes blood donors from ever being infected. And yet we are told some are infected and their infection proves AIDS infectious. Thirdly, the method excludes the very large set of individuals who are not infected with HIV but who have exactly what confounds antibody tests. More than their share of antibodies. Potentially cross-reacting or non-specifically induced antibodies.
NO RISK HOSPITAL PATIENTS
St. Louis 1988HOS NUM ALL MEN 25-44 WOM 25-44 1 2897 7.8 21.7 7.4 2 4406 5.6 18.4 7.8 3 1968 3.2 13.3 3.5 4 1720 1.9 7.1 0.7 5 5380 0.9 3.2 0.8 6 3299 2.6 7.7 3.3 7 3823 1.9 1.8 2.4 8 4275 1.8 5.7 0.8 If you do study such patients, but not those at risk for AIDS, you can see that considerable numbers are antibody positive, and more so if the person is Black or Hispanic. This study examined blood specimens from 90,000 hospital patients where the authors excluded even patients with knife and gun shot wounds because such patients do have a slightly increased risk of being HIV positive. They found up to 22% of men and 8% of women aged 25-44 with antibodies. This included on the confirmatory Western blot. These figures from North Eastern United States rival some parts of Africa. Are these people infected with HIV? Ten years later had these no risk young men and women developed or died of AIDS? These patients are sick but sick in the affluent US and in hospital. But I bet there are also patients like this in Africa who are a lot sicker, who are tested with just one ELISA and no confirmatory Western blot. And theyre not in hospital.
Possibly the most significant study looking at the specificity of the HIV antibody tests was published by Colonel Donald Burke from the US Army. He took the exact opposite premise from Gallo and said healthy people can be infected with HIV. He chose 135,187 young, low risk applicants for military service and came up with these data.
HIV No HIV Positive 14 1 Negative 0 135172 14 135173
Total 135187 Sensitivity 100% Specificity 99,9993% Burke discovered 15 seropositives and regarded all but one HIV infected. That gave him a specificity of, to use his own words, roughly 99.9993%. What is revealing is how Burke defined his soldiers HIV positive and how he determined which of those were truly HIV infected.
HIV Positive 2E + 2WB HIV Negative Not above Truly infected 2E + 2WB + 4XWB Not truly infected Not above Soldiers were HIV positive if they had two positive ELISAs and two positive WBs. Anything less was not positive.
The method used to prove true infection was to perform four additional antibody tests on the 15 soldiers found HIV positive. These were other brands of the WBs or equivalent tests. A soldier who was positive on a total of 8 antibody tests was declared truly infected. Any less and he wasnt. This can only be described as bizarre. Yet this paper was lauded in an editorial in the New England Journal of Medicine.
And what do you tell a 17 year old antibody positive civilian blood donor tested with Gallos ELISA who the next day joins the Army and reacts another seven times under the auspices of Donald Burke?
The facto gold standards are:
- The clinical syndrome
- Low risk/good health
- Repeating the test
You cannot use de facto gold standards for proving the presence or absence of HIV infection.
Where does this leave us?
AIDS No AIDS AB Pos. AB Neg. It is perfectly reasonable to correlate AIDS or non-AIDS with these tests. Amongst the risk groups these tests obviously mean something.
HIV No HIV AB Pos. AB Neg. Presently, nowhere in the scientific literature are there data with which to complete above table. And until these data are forthcoming, we cannot claim to know what proportion, if any, antibody positive people are HIV infected.
Currently available HIV antibody tests are extraordinarily accurate, both in terms of sensitivity (the ability of the test to give a positive finding when a subject is truly HIV-infected) and specificity (the ability of the test to give a negative finding when a subject is truly HIV-free). -- NIAID websiteWhich puts the Perth group as at odds with the most of you, the World Health Organisation, the NIH, and others too numerous to mention.
But possibly not with Abbott Laboratories.
At present there is no recognized standard for establishing the presence or absence of HIV-1 antibody in human blood -- Abbott Laboratories 1988, 1998What relevance does our interpretation of the scientific literature hold for South Africa? From our perspective would seem reasonable to suggest a moratorium on antibody testing until the specificity of the HIV proteins and the antibody reactions to these proteins has been sorted out. If this seems too radical for HIV protagonists then perhaps a compromise would be not to react virologically to positive tests. By that I mean refraining from measuring viral load or administering anti-retroviral drugs. Sometime ago Professor Makgoba wrote an article stressing the importance of solving scientific problems by putting hypotheses and proposing experiments. We thank him for this suggestion and have already posted suggested experiments to the Internet debate website (The Perth group contributions to the Internet debate that followed the first Presidential Panel meeting can be read at www.deltav.apana.org.au/~vturner/aids). In regard to the specificity problem one of these experiments is worth mentioning. Absorb antibody positive sera with mycobacterial and fungal and auto antigens. If the antibody reactivity diminishes or disappears then HIV antibodies must be regarded non-specific and cannot be used to prove HIV exists in AIDS patients. This is a very simple experiment and if the predicted outcome eventuates, the HIV theory will become untenable.
Thank you.
The real purpose of scientific method is to make sure Nature hasn't misled you into thinking something you don't actually know... One logical slip and an entire scientific edifice comes tumbling down. One false deduction about the machine and you can get hung up indefinitely. -- Robert Pirsig, Zen and the Art of Motorcycle Maintenance