THE CAUSES OF AIDS By Roberto Giraldo
June 2000
1. A Proposal for the Phisiological Pathogenesis of AIDSFive types of immunological stressor agents can alter the functioning of the immune system: chemical, physical, biological, mental, and nutritional. Numerous facts illustrate the incremental growth of these agents in recent decades, as well as their diversity throughout countries and continents (1-3).
Our soil, water, air, and food are polluted with numerous chemical, physical, biological, and nutritional stressors. We are all exposed to stressor agents either involuntarily through the conditions under which we are obligated to live or voluntarily through life styles that we have chosen (1-3).
AIDS occurs in groups of people who ¾ through their living conditions or life styles ¾ are more heavily exposed than others to the multiple, repeated, and chronic actions of immunological stressor agents (4-11).
These stressors can produce toxicity (immunotoxic effect) and can activate the regular molecular and cell networks (immunogenic effect) when acting on immunocompetent cells. Both immunotoxic and excessive immunogenic effects (over stimulation of immune responses) induce degeneration of cells and the functioning of the immune system (7-10).
AIDS is the most severe of all acquired immunodeficiencies, secondary to multiple, repeated, and chronic exposures to immunological stressors. These progressive and continuous deleterious actions upon the immune system bring the individual to a collapse of immunological functions, with the subsequent and simultaneous appearance of infections, neoplasias, and metabolic disturbances. In addition to acting upon the immune system, stressor agents alter functioning of practically all other bodily systems and organs.
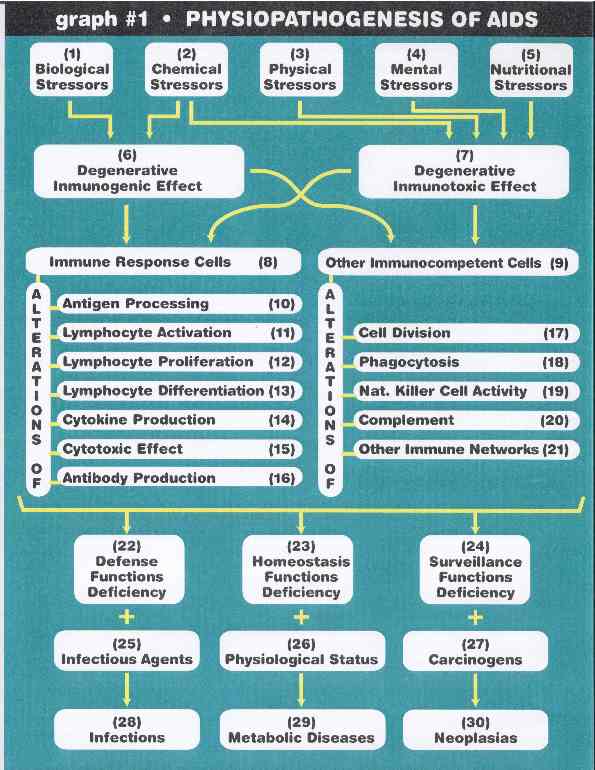
Graph #1 shows a schematic summary of this proposal for the physiopathogenesis of AIDS (7,9).
Chemical [2] and biological [1] stressors produce degenerative-immunogenic effects [6] on immunocompetent cells. On the other hand, physical [3], mental [4], nutritional [5], and chemical [2] stressors, produce degenerative-immunotoxic effects [7] on these same cells.
The immunogenic [6] and immunotoxic [7] effects on cells involved in the immune response [8] are responsible for a variety of alterations upon different steps of the immune response, such as; disturbances in antigen processing [10], lymphocyte activation [11], lymphocyte proliferation [12], lymphocyte differentiation [13], cytokine production [14], cytotoxic effect [15], and antibody production [16].
Additionally, the immunogenic [6] and immunotoxic [7] effects on other immunocompetent cells, those of the bone marrow, peripheral blood, and other tissues, are translated into a variety of alterations in cell division [17], phagocytosis [18], natural killer-cell activity [19], complement system [20], and other immune networks [21], also related to the immune response.
The severe physiological alterations of cells involved in the immune response [8], as well as alterations of other immunocompetent cells [9], are responsible for the deficiency of the three main functions of the immune system: defense [22], homeostasis [23], and surveillance [24].
Following this, certain infectious agents [25] find a unique opportunity to grow within the deficiency of the defensive functions [22], and generate a variety of infectious diseases [28], termed opportunistic infections. The deficiency of the homeostasis functions [23], depending on the physiological status of the tissues and organs of the individual [26], can be responsible for a variety of metabolic disturbances and conditions [29]. The deficiency in surveillance functions, together with the presence of carcinogen agents and all other factors involved in the carcinogenesis process, are responsible for the occurrence of neoplasias [30].
2. A Proposal for the Molecular Pathogenesis of AIDS
At a molecular level, AIDS is caused by the accumulation of free radicals, especially oxidizing agents, in all systems, organs, and tissues, but principally within the cells and chemical reactions of the immune system (4,8,10-22). As a consequence, the clinical manifestations of AIDS ¾ opportunistic infections, tumors, and metabolic disturbances and conditions ¾ as well as the severity of the illness are directly proportional to the levels of free radicals, especially oxidizing agents in the tissues of the AIDS patient.
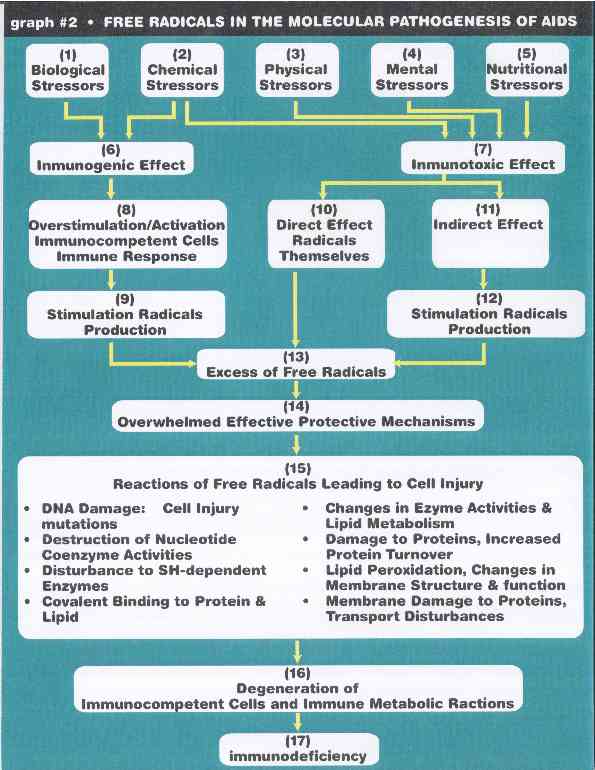
Graph #2 is a illustration of this proposal (7,9).
Chemical [2] and biological [1] stressors, through an immunogenic effect [6] with an over stimulation/activation of immunocompetent cells of the immune response [8], stimulate the production of free radicals [9]. On the other hand, physical [3], mental [4], nutritional [5], and chemical [2] stressors cause an immunotoxic effect [7], either by acting directly as free radicals themselves [10], or through an indirect effect [11] can stimulate their production [12], contributing to a critical excess of free radicals [13]. The excess of radicals, together with over-saturation of the oxidation protective mechanisms [14], causes damage to immunocompetent cells through different chemical reactions [15], with degeneration of immunocompetent cells and reactions [16]. As a result, a collapse of all immunological functions will manifest itself with the subsequent and simultaneous appearance of opportunistic infections, metabolic conditions, and neoplasias. In other words, AIDS [17].
3. A Proposal for the Definition of AIDS
I propose to define AIDS as a toxic and nutritional syndrome, the most severe and profound of all acquired immunodeficiencies, due to multiple, repeated, and chronic exposures to immunological stressor agents. These stressors cause degenerative immunotoxic and immunogenic effects on immune cells and reactions, with the accumulation of free radicals, especially oxidizing agents, in all body systems but principally in the organs and tissues of the immune system. These progressive and continuous deleterious actions upon the immune system bring the individual to a collapse of immunological functions, with the subsequent and simultaneous appearance of infections, neoplasias, and metabolic conditions. Simultaneous with acting on the immune system, stressor agents alter the functioning of practically all other systems and organs. The continuation of this process eventually causes the death of the person (7-10).
The diverse clinical manifestations of AIDS are the direct consequence of the physiologic and molecular pathogenesis of the syndrome. The distribution of immunological stressors varies within the groups of people at risk for AIDS. This fact is the primary explanation for the great deal of variation in the clinical manifestations of AIDS within the groups of people at risk for it. While altering the immune system, the exposure to stressor agents also causes damage to practically all systems, organs and tissues of the body. This is another factor in explaining the great deal of variety in the clinical manifestations of AIDS within the groups at risk for it. In AIDS, not only the immune system collapses, but all other systems as well (7-10).
In brief, AIDS is neither an infectious disease nor is sexually transmitted. It is a toxic and nutritional syndrome caused by the alarming worldwide increment of immunological stressor agents.
This article was written in June 2000 and posted during the Internet Discussion of the South African Presidential AIDS Advisory PanelReferences
- Giraldo RA. AIDS and Stressors I: Worldwide Rise of Immunological Stressors. Toxicology Letter Supplement 1/78. 1995: s34.
- Giraldo RA. AIDS and Stressors I: Worldwide Rise of Immunological Stressors. In: AIDS and Stressors: AIDS is Neither an Infectious Disease nor is Sexually Transmitted. It is a Toxic-Nutritional Syndrome Caused by the Alarming Worldwide Increment of Immunological Stressor Agents. Medellín, Colombia: Impresos Begón, 1997: 23-56.
- Giraldo RA. El Alarmante Incremento Mundial de Agentes Estresantes Inmunologicos. In: Ahumada C, et al. Relaciones Internacionales, Politica Social y Salud: Desafios en la Era de la Globalización. Bogotá, Colombia: Fundación Cultural Javeriana, 1998: 49-73.
- Papadopulos-Eleopulos E. Reappraisal of AIDS – Is the Oxidation Induced by the Risk Factors the Primary Cause? Medical Hypothesis 1988; 25: 151-162.
- Duesberg PH. AIDS Acquired by Drug Consumption and other Noncontagious Risk Factors. Pharmac Ther 1992; 55:201-277.
- Duesberg PH, Rasnick D. The AIDS Dilema: Drug Diseases Blamed on a Passenger Virus. Genetica 1998; 104: 85-132.
- Giraldo RA. AIDS and Stressors II: A Proposal for the Pathogenesis of AIDS. Toxicology Letter Supplement 1/78. 1995: s34.
- Giraldo RA. AIDS and Stressors III: A Proposal for the Natural History of AIDS. Toxicology Letter Supplement 1/78. 1995: s35.
- Giraldo RA. AIDS and Stressors II: A Proposal for the Pathogenesis of AIDS. In: AIDS and Stressors: AIDS is Neither an Infectious Disease nor is Sexually Transmitted. It is a Toxic-Nutritional Syndrome Caused by the Alarming Worldwide Increment of Immunological Stressor Agents. Medellín, Colombia: Impresos Begón, 1997: 57-96.
- Giraldo RA. AIDS and Stressors III: A Proposal for the Natural History of AIDS. In: AIDS and Stressors: AIDS is Neither an Infectious Disease nor is Sexually Transmitted. It is a Toxic-Nutritional Syndrome Caused by the Alarming Worldwide Increment of Immunological Stressor Agents. Medellín, Colombia: Impresos Begón, 1997: 97-131.
- Giraldo RA, et al. Is It Rational to Treat or Prevent AIDS With Toxic Antiretroviral Drugs in Pregnant Women, Infants, Children, and Anybody Else? The Answer is Negative. Continuum (London) 1999; 5(6): 38-52.
- Dworkin B, et al. Selenium Deficiency in the Acquired Immuno-Deficiency Syndrome. J Parenteral Enteral Nutr 1986; 10:405.
- Fabris N, et al. AIDS, Zinc Deficiency and Thymic Hormone Failure. JAMA 1988; 259: 839.
- Papadopulos-Eleopulos E. Looking Back on the Oxidative Stress Theory of AIDS. Continuum (London) 1998/9; 5(5): 30-35.
- Papadopulos-Eleopulos E, et al. Oxidative Stress, HIV and AIDS. Res Immunol 1992; 143: 145-148.
- Turner VF. Reducing Agents and AIDS – Why Are We Waiting? Med J Austr 1990; 153: 502.
- Favier A. The Place of Oxygen Free Radicals in HIV Infections. A collection of papers presented at a conference on "The place of oxygen free radicals in HIV infection", Les Deux Alpex, France, January 1993. Chem Biol Interac 1994; 91: 91-100.
- Salvain B, Mark AM. The Role of Oxidative Stress in Disease Progression in Individuals Infected by the Human Immunodeficiency Virus. J Leukocyte Biol 1992; 52: 111.
- Greenspan HC. The Role of Oxidative Oxygen Species, Antioxidants and Phytopharmaceuticals in Human Immunodeficiency Virus Activity. Med Hypothesis 1993; 40: 85.
- Piette J et al. Molecular Mechanisms of Virus Activation by Free Radicals. Collection of 5 articles presented at a conference on "The place of oxygen free radicals in HIV infection", Les Deux Alpes, France, January 1993. Chemico-Biological Interactions 1994; 91: 79-132.
- Shallenberger F. Selective Compartimental Dominance: An Explanation for a Noninfectious Multifactorial Etiology for Acquired Immune Deficiency Syndrome (AIDS), and a Rationale for Ozone Therapy and Other Immune Modulating Therapies. Med Hypothesis 1998; 50: 67-80.
- Passi S. Progressive Increase of Oxidative Stress in Advancing Human Immunodeficiency. Continuum (London) 1998; 5(4): 20-26.